These usually present with lymphadenopathy with or without systemic symptoms similar to Diffuse Large B-cell Lymphoma (DLBCL).
Advanced stage disease and extranodal involvement may be more common than DLBCL.
Diagnosis
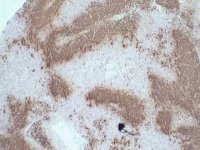
There is infiltration and replacement of the normal nodal or other tissue
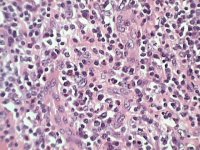
The tumour cell morphology is highly variable but most cases have a mixture of medium and large lymphoid cells showing highly irregular nuclei
The phenotype is typically:
CD3+, CD2+, CD5+, CD4+, CD45RO+ but there is variation between cases
large number of reactive cells including macrophages, eosinophils and plasma cells may be present in some cases.
Treatment and Outcome
Most patients are treated initially with CHOP or similar type combination chemotherapy.
The overall outcome is poor reflecting presentation with advanced stage disease and more aggressive behaviour of T-cell lymphomas. A small group of patients has a more indolent course.
Angio-immunoblastic type peripheral T-cell lymphoma is a distinctive clinico-pathological entity. Many of the features are presumed to be due to abnormal secretion of cytokines by the tumours cells. Some patients may have systemic symptoms that appear out of proportion to the apparent disease bulk.
Diagnosis
The diagnosis requires lymph node biopsy. The nodal architecture is replaced by:
neoplastic cells which are medium sized T-cells, usually with a small proportion of larger blast cell. These are CD4+ peripheral T-cells and may have an abnormal phenotype. A small number of cells may contain Epstein-Barr virus, the significance of this is uncertain.
Systemic symptoms may be present in some patient with extensive disease.
Diagnosis
In typical cases the cells are very large with abundant cytoplasm, often with a distinctive golgi, large nuclei with prominent nucleoli. Multi-lobated cells are frequent. A number of morphological variants are described.
The cells are strongly CD30+ and CD45+ and have variable expression of pan-T-cell markers.
The t(2;5) is a key diagnostic feature of anaplastic large cell lymphoma. This results in a fusion protein NPM-ALK which has abnormal kinase activity.
The t(2;5) is found in younger patients and tumours with this translocation have a much better outcome.
It is essential to differentiate this tumour from CD30+ cutaneous large cell lymphoma. This is complicated by the relatively frequent involvement of the skin in systemic anaplastic large cell lymphoma.
Treatment and Outcome
Initial treatment is usually with CHOP type combination chemotherapy.
This is critically dependant on the t(2;5). Tumour with the translocation have >70% 5 year survival. Those without the t(2;5) have a 25% 5 year survival. This effect suggests that the t(2;5) tumours should be regarded as a separate entity.
The outcome also depends on the International Prognostic Index