![]()
 |
 |
 |
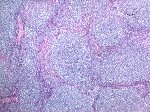
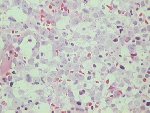
A follicular growth pattern |
A mixture of centrocytes and centroblasts |
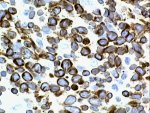
Aberrant expression of bcl-2 indicative of the t(14,18) |
 |
 |
Three-colour flow cytometric analysis of lymph node cells for a typical case of follicle centre lymphoma. A proportion of cells express CD10 in combination with CD38. There is light chain restriction with almost all the cells expressing sIg-kappa. The other main immunophenotypic features are the presence of either IgM or IgG with CD19, CDw75 and CD20. CD23 is present in some cases. CD45RA is often aberrantly expressed in follicle centre lymphoma. |
|
 |
bcl-2/IgH PCR in a series of bone marrow samples from patients with follicular centre lymphoma. A rearranged band is seen in lanes 2, 3, 4, 5, 8 & 9. Lane 11 is a standard. The varying size of the band illustrates the variation in breakpoints between patients. |
![]()
 |
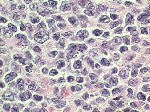
Transformed follicle centre lymphoma. In this case the patient had clinical features of acute leukaemia with marrow replacement by large lymphoid blast cells with the phenotype sIg-kappa+, CD19+, CD10+, CD23- |
![]()
![]()
Comments & feedback to: admin@hmds.org.uk