[ Home Page ] [ Site Map ]
Marginal Zone Lymphoma and Waldenstrom's Macroglobulinaemia
I) Marginal Zone Lymphoma
II) Waldenstrom's Macroglobulinaemia and Lymphoplasmacytoid Lymphoma
The normal marginal zone is most prominent in lymphoid tissue in the spleen and at extranodal sites. It consists of post-germinal centre memory B-cells.
Marginal zone lymphoma has three distinct clinical presentations:
- Localised extranodal disease - stomach, intestine, thyroid, skin and salivary glands
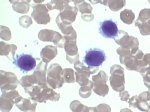
- Splenic marginal zone lymphoma with or without circulating villous lymphocytes and marrow disease
- Solitary nodal disease; this is sometimes associated with occult extranodal involvement
Lymphoplasmacytoid lymphoma and Waldenstrom's macroglobulinaemia show similar cellular features and may be closely related.

A) Morphology
- Mixture of centrocyte-like cells, monocytoid B-cell, plasmacytoid cells and blasts
- Invade and replace existing reactive germinal centres
- Invade and destroy epithelium at extranodal sites - lympho-epithelial lesions
- At extranodal sites the lymphoma often appear to be developing in the context of chronic inflammation.
 |
 |
 |
Romanowski-stained peripheral blood smear - splenic lymphoma with villous lymphocytes. |
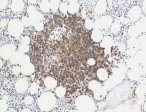
Bone marrow stained by CD20-immunoperoxidase showing nodular infiltrate of MZL cells |
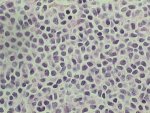
Bone marrow trephine biopsy stained with H & E showing extensive infiltration. |
 |
 |
 |
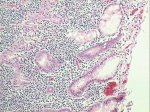
Lymph node section stained with H & E. |
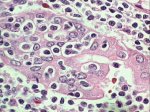
MZL infiltration of stomach mucosa, showing formation of lympho-epithelial lesions. |
MZL lympho-epithelial lesion from stomach mucosa infiltrate - high power magnification. |
B) Immunophenotype
- sIgM (rarely IgD), CD20+, CD19+, CD10-, CD5-, CD23-
- Hypermutation of immunoglobulin genes is present consistent with the post-germinal centre phenotype. Difference in the extent of intra-clonal heterogeneity is seen in different subtypes.
- Trisomy 3 is the commonest numerical chromosomal abnormality found in up to 70% of cases, together with trisomy 18 and rearrangement of chromosome 1
- The pattern of numerical chromosomal abnormalities is similar in nodal and extranodal disease.
- The t(11;18) appears to be present in 50% of cases of extranodal marginal zone lymphoma. Its incidence in nodal cases is currently unknown.
- t(1;14) with re-arrangement of bcl-10 occurs in a small proportion of cases.
- Both t(11;18) and t(1;14) appear to have an anti-apoptotic effect.
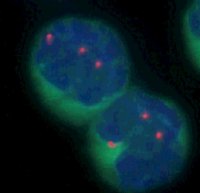 |
FISH image demonstrating Trisomy 3, the commonest cytogenetic abnormality in marginal zone lymphoma. |
Extranodal marginal zone lymphoma
- Frequently arises in the context of chronic inflammation
- May be localised or multifocal
- Disease bulk varies widely
- May transform to diffuse large B-cell lymphoma but incidence is not certain. Cytogenetic studies suggest that the majority of extranodal diffuse large B-cell lymphoma may arise de novo
Gastric marginal zone lymphoma and Helicobacter pylori
- Gastric marginal zone lymphoma occurs almost exclusively in the context of Helicobacter pylori infection
- May be localised, multifocal or diffuse Endoscopic ultrasound may be useful in assessing the extent of infiltration of the gastric wall.
- Regression and stable remission of disease frequently follows Helicobacter eradication.
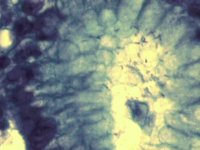 |
Helicobacter pylori in section of gastric mucosa; Giemsa stain |
- The overall survival for patients with extranodal marginal zone lymphoma is 80-100%. Deaths from disease are rare.
- Gastric marginal zone lymphomas not responsive to Helicobacter eradication or tumours at other sites may be treated with single agent chemotherapy. Very little data on outcome is available. The role of radiotherapy after complete surgical removal is not certain.
- The overall survival of patients with splenic lymphoma with villous lymphocytes is 78% at 5 years. Splenectomy or single agent chemotherapy are used but there is little data from controlled trials.
- Nodal disease is treated with chlorambucil and in most cases has an indolent clinical course, although definitive data is sparse.
Clinical Features
- The key feature of Waldenstrom's macroglobulinaemia is the presence of an IgM paraprotein. This may act as a cold agglutinin or be associated with haemolysis
- The clinical features are otherwise similar to splenic marginal zone lymphoma/SLVL.
Laboratory Diagnosis
- Highly variable degree of marrow infiltration that may have an interstitial or diffuse pattern
- Morphology and phenotype is similar to that seen in marginal zone lymphoma
- The term Lymphoplasmacytoid lymphoma includes Waldenstrom's and some identical cases without a paraprotein or typical features of SLVL.
It is likely that lymphoplasmacytoid lymphoma, Waldenstrom's, SLVL, nodal and splenic marginal zone lymphoma all represent variants of a systemic form of marginal zone lymphoma. The diagnostic term used often reflects the initial clinical presentation rather than significant differences in the cellular features or the pattern of disease.
[ Home Page ] [ Site Map ]
Copyright © HMDS 1999-2005
Document last updated:
Tuesday, 18 November 2003
Comments & feedback to:
admin@hmds.org.uk
[URL: www.hmds.org.uk/mzl.html]